Academic Article, January 2026
Hereditary Gynecologic Cancers:
What Clinicians Should Recognize in Daily Practice
Sopita Prasertpakdi, M.D.
Asst.Prof. Kittipat Charoenkwan, M.D.
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology,
Faculty of Medicine, Chiang Mai University, Thailand
Why hereditary gynecologic cancer matters?
Gynecologic cancers represent a major health burden among women worldwide. While most cases arise sporadically, a clinically significant proportion are attributable to inherited cancer predisposition syndromes. Hereditary gynecologic cancers account for approximately 5– 10% of ovarian cancers(1) and 3–5% of endometrial cancers(2), yet their impact extends far beyond these numbers. Failure to recognize hereditary risk can result in missed opportunities for early detection, risk-reducing interventions, and cancer prevention among affected family members.
Importantly, identification of hereditary cancer risk does not rest solely within the domain of geneticists or subspecialists. Physicians across disciplines —particularly those in primary care, internal medicine, and general obstetrics and gynecology—play a pivotal role in recognizing clinical patterns that warrant further evaluation. This article aims to provide a practical, clinician-focused overview of hereditary gynecologic cancers, emphasizing recognition, clinical red flags, and appropriate next steps in routine practice.
Key Hereditary Syndromes Shaping Gynecologic Cancer Risk
Hereditary Breast and Ovarian Cancer Syndrome (HBOC)
Hereditary Breast and Ovarian Cancer (HBOC) syndrome is the most recognized inherited cancer syndrome affecting gynecologic organs. Awareness of hereditary cancer risk increased markedly following the “Angelina Jolie effect.”(3) HBOC is strongly associated with ovarian, fallopian tube, and primary peritoneal cancers, as well as breast cancer. Ovarian cancers in this
setting are typically high-grade serous carcinomas and often present at a younger age than sporadic cases.(4)
Clinically, ovarian cancer at any age should raise suspicion for HBOC, especially when accompanied by a personal or family history of breast cancer, early-onset disease, or multiple affected relatives. Given the rarity of ovarian cancer, even a single case in a family warrants hereditary risk assessment.
Lynch Syndrome
Lynch syndrome is an autosomal dominant hereditary cancer syndrome caused by germline pathogenic variants in DNA mismatch repair (MMR) genes—MLH1, MSH2, MSH6, PMS2— or deletions involving the EPCAM gene. It affects approximately 1 in 300 individuals and confers a lifetime cancer risk ranging from 10% to 90%, depending on the specific gene variant and cancer type. Individuals with Lynch syndrome are predisposed to multiple malignancies, most commonly endometrial and colorectal cancers, but also including ovarian, gastric, small bowel, urinary bladder and etc.(5)
In affected women, endometrial cancer often serves as the sentinel malignancy, frequently preceding the diagnosis of colorectal cancer.(6) Lynch-associated endometrial cancers typically present at a younger age and may occur in the absence of traditional risk factors, such as obesity or prolonged estrogen exposure.
Ovarian cancer may also develop in Lynch syndrome, often at a younger age than sporadic cases and commonly exhibiting non-serous histologic subtypes. Recognition of these characteristic clinical and pathologic patterns is crucial, as early identification enables targeted surveillance and preventive strategies for endometrial, colorectal and other associated malignancies. (7)
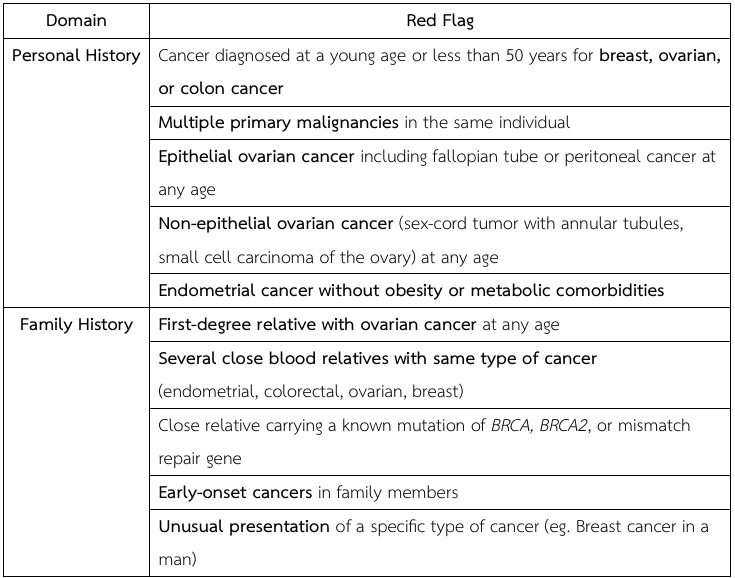
Red Flags in Personal and Family History (8, 9)
Clinical Evaluation and Management of Suspected Hereditary Cancer Risk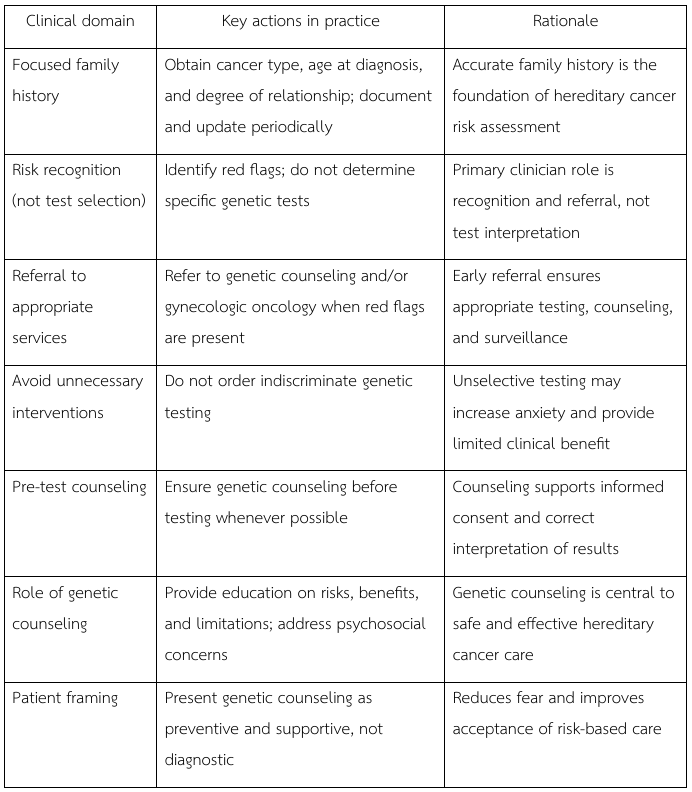
References
- Lu Hereditary gynecologic cancer: risk, prevention and management: CRC Press; 2008.
- Daniels Genetic testing by cancer site: uterus. Cancer J. 2012;18(4):338-42.
- Evans DG, Barwell J, Eccles DM, Collins A, Izatt L, Jacobs C, et The Angelina Jolie effect: how high celebrity profile can have a major impact on provision of cancer related services. Breast Cancer Res. 2014;16(5):442.
- Schrader KA, Hurlburt J, Kalloger SE, Hansford S, Young S, Huntsman DG, et Germline BRCA1 and BRCA2 mutations in ovarian cancer: utility of a histology-based referral strategy. Obstet Gynecol. 2012;120(2 Pt 1):235-40.
- Underkofler KA, Ring Updates in gynecologic care for individuals with lynch syndrome. Front Oncol. 2023;13:1127683.
- Lu KH, Dinh M, Kohlmann W, Watson P, Green J, Syngal S, et Gynecologic cancer as a “sentinel cancer” for women with hereditary nonpolyposis colorectal cancer syndrome. Obstet Gynecol. 2005;105(3):569-74.
- Ketabi Z, Bartuma K, Bernstein I, Malander S, Grönberg H, Björck E, et Ovarian cancer linked to Lynch syndrome typically presents as early-onset, non-serous epithelial tumors. Gynecol Oncol. 2011;121(3):462-5.
- Lancaster JM, Powell CB, Chen LM, Richardson Society of Gynecologic Oncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol. 2015;136(1):3-7.
- Hereditary Cancer Syndromes and Risk Assessment: ACOG COMMITTEE OPINION, Number Obstetrics & Gynecology. 2019;134(6):e143-e9.