Academic Article, February 2026
Postmenopausal Bleeding: Clinical Approach and Management
Khemanat Khemaworapong, MD, Asst. Prof. Bunlert Wiriyapak, MD
Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital
Postmenopausal Bleeding (PMB) is a common gynecological issue encountered in general practice, accounting for approximately 5% of all gynecological visits. It is clinically defined as vaginal bleeding occurring at least 12 months after a woman’s last menstrual period.
The clinical significance of PMB lies in its role as the primary “Red Flag Sign” for Endometrial Cancer. Studies indicate that over 90% of endometrial cancer patients present with this symptom. However, from an epidemiological perspective, the majority of PMB cases are caused by benign conditions. The incidence of endometrial cancer in patients presenting with PMB is only 10% or less. Therefore, General Practitioners play a crucial role in history taking, physical examination, and initial triage to identify high-risk patients for timely referral and treatment.
Etiology and Pathophysiology
Physiological changes during menopause result from the cessation of ovarian function, leading to permanently low levels of estrogen and progesterone. While the causes of PMB can be classified using the FIGO PALM-COEIN system, the common differential diagnoses in clinical practice for postmenopausal women include:
Atrophic Endometrium: This is the most common cause with about 60-80% incidence. It results from estrogen deficiency, causing the endometrial lining to become thin, dry, and fragile, leading to micro-fissures and subsequent bleeding.
Endometrial Polyps: Common benign proliferations of the endometrium occupying 2-12% causes of bleeding which may not respond to hormonal treatment.
Endometrial Hyperplasia & Carcinoma: Both diseases involve only 15-20% of all causes but they are the most critical conditions to rule out. Major risk factors include unopposed estrogen (e.g., in patients with obesity, PCOS, or estrogen-only HRT), advanced age, diabetes, and hypertension.
Exogenous Hormones: About 15-25% of postmenopausal bleeding can be caused by Hormone Replacement Therapy (HRT) or specific medications like Tamoxifen, which has a proliferative effect on the endometrium.
Clinical Evaluation
History Taking: Physicians should assess risk factors and differentiate potential causes:
Bleeding Characteristics: Duration, volume (spotting vs. heavy flow), and precipitating factors.
Gynecologic History: Date of Last Menstrual Period (LMP), history of HRT use, and Pap smear history.
Risk Factors for Endometrial Cancer: Obesity (BMI > 30), diabetes, hypertension, nulliparity, or a family history of Lynch syndrome.
Medications: particularly anticoagulants or herbal supplements.
Physical Examination: A pelvic examination is mandatory to exclude non-uterine sources of bleeding:
Vulva/Vagina: Assess for signs of atrophy, lacerations, or trauma.
Cervix: Check for cervical polyps or signs of cervical cancer (perform Pap smear/HPV testing if not up to date).
Uterus/Adnexa: Palpate for uterine size and adnexal masses.
Diagnostic Imaging & Workup
The core of PMB management is the evaluation of the endometrium to determine the need for invasive procedures. Transvaginal Ultrasonography (TVUS) is the highly effective and cost-efficient first-line modality. Physicians should order a TVUS to measure the Endometrial Thickness (EMT). The EMT should be measured in the sagittal view, capturing the maximum double-layer thickness, excluding any intracavitary fluid.
Interpretation Guidelines (Cut-off Value):
EMT ≤ 4 mm: This finding has a Negative Predictive Value (NPV) of 99% for endometrial cancer. The risk of malignancy is extremely low. Physicians may consider expectant management or treat for atrophy without immediate biopsy.
EMT > 4 mm: Considered a “Thickened Endometrium.” Tissue sampling is required for pathological evaluation.
Focal Abnormality / Irregularity: Even if the EMT is thin (< 4 mm), if the lining appears irregular or a focal lesion is visualized, further investigation is indicated.
If TVUS is abnormal (EMT > 4 mm) or if the patient has persistent bleeding despite normal
Endometrial Biopsy (Office-based): Currently the Gold Standard. It can be performed in the outpatient setting using a suction device (e.g., Pipelle). It offers high sensitivity, is cost-effective, and requires no anesthesia.

Picture showed a sample of Pipelle.
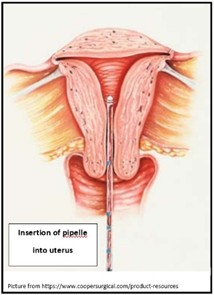
Picture showed intrauterine aspiration (endometrial sampling).
Saline Infusion Sonography (SIS): Instilling saline into the uterine cavity helps distinguish between diffuse endometrial lesions (e.g., hyperplasia) and focal lesions (e.g., polyps or submucous myomas), aiding in surgical planning.
Hysteroscopy: This method provides the highest diagnostic accuracy. It is recommended when: Office biopsy yields inadequate tissue or cannot be performed (e.g., cervical stenosis). Bleeding persists despite normal biopsy results. A focal lesion is suspected on TVUS/SIS, allowing for simultaneous therapeutic polypectomy.
Management Principles
1. Atrophic Endometrium: Observation is acceptable. If bleeding persists, Topical Estrogen can be prescribed to restore tissue moisture and integrity.
2. Endometrial Polyps: Polypectomy (via Hysteroscopy) is recommended to relieve symptoms and obtain pathological confirmation.
3. Endometrial Hyperplasia:
Without Atypia: Treat with Progestin therapy (Oral or LNG-IUD).
With Atypia: Consider Hysterectomy due to the high risk of progression to cancer or co-existing malignancy.
4. Endometrial Cancer: Refer to a Gynecologic Oncologist for staging surgery (Hysterectomy + Bilateral Salpingo-Oophorectomy +/- Lymph node assessment).
Conclusion
Postmenopausal Bleeding is a symptom that always requires investigation. While the majority of cases are benign, the primary clinical objective is the exclusion of endometrial cancer. Transvaginal Ultrasound is an effective screening tool; utilizing an EMT cut-off of ≤ 4 mm helps reduce unnecessary invasive procedures. However, in high-risk cases or persistent symptoms, Endometrial Biopsy remains the essential standard for diagnosis.
References
Hurtado S, Shetty MK. Post-Menopausal Bleeding: Role of Imaging. Semin Ultrasound CT MR. 2023 Dec;44(6):519-527.
Papakonstantinou E, Adonakis G. Management of pre-, peri-, and post-menopausal abnormal uterine bleeding: When to perform endometrial sampling? Int J Gynaecol Obstet. 2022 Aug;158(2):252-259.
Gatenby C, Simpson P. Menopause: Physiology, definitions, and symptoms. Best Pract Res Clin Endocrinol Metab. 2024 Jan;38(1):101855.